Von Willebrand disease overview
Last updated July 2, 2025, by Marisa Wexler, MS
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
Von Willebrand disease (VWD) is a bleeding disorder in which the body cannot properly form blood clots, leading to abnormally heavy and prolonged bleeding. It is usually caused by genetic mutations that a person has inherited from their parents and is born with.
VWD cannot be cured, but there are a range of treatments available that can help people with VWD keep bleeding under control and manage other disease symptoms.
What is von Willebrand disease?
VWD is a bleeding disorder in which blood clotting is impaired, resulting in abnormal bleeding. The manifestations of VWD are similar to those seen in hemophilia, another bleeding disorder, though its symptoms are typically less severe.
VWD is the most common bleeding disorder, estimated to affect up to 1% of people in the U.S., though many individuals with the disease have mild or no symptoms at all. Only about 0.01% of people in the world have VWD that causes clinically significant symptoms. Unlike hemophilia, which is more commonly seen in men, VWD affects men and women equally.
Causes and risk factors
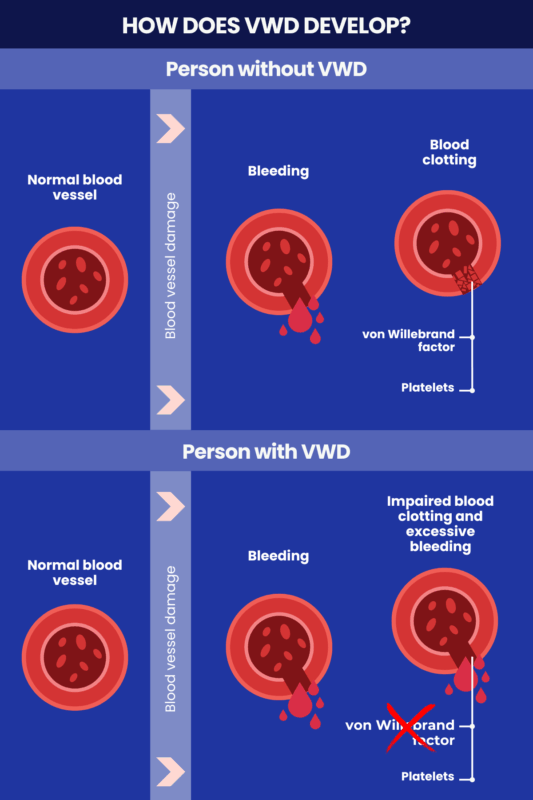
Von Willebrand factor (VWF) is a protein that helps the blood to clot. It normally acts like a glue to help cell fragments called platelets stick together and form a clot at the site of injury to stop bleeding. VWF also helps stabilize and transport factor VIII (FVIII) to the site of injury to promote blood clotting. FVIII is another clotting factor, or protein that is important for blood clotting.
In VWD, there’s a lack of functional VWF — either because protein levels are too low, or because the protein is dysfunctional — impairing the clotting process.
The VWF protein is encoded by the VWF gene. The most common VWD causes are mutations in this gene that are inherited from a person’s biological parents.
Everyone inherits two copies of the VWF gene, one from each parent. Some types of VWD are inherited in an autosomal dominant manner, meaning that one mutated gene copy is sufficient to cause the disease. Other forms are inherited in an autosomal recessive manner, meaning that both gene copies must be faulty for the disease to manifest.
- In autosomal dominant inheritance, a person has a 50% chance of passing the disease-causing mutation on to their biological children.
- In autosomal recessive inheritance, if two people who each carry a mutated copy of the gene have a child, there’s a 25% chance that the child will inherit both mutated copies and develop the disease.
In rare cases, VWD may be caused by mutations that arise spontaneously, rather than being inherited.
Although VWD is typically inherited, there are also rare cases where the disease develops later in life as a consequence of other diseases or medications that lead to low VWF activity levels. This is known as acquired von Willebrand syndrome (AVWS). Possible causes of AVWS include:
- disorders where immune cells grow excessively, including some blood cancers like leukemia and multiple myeloma
- autoimmune disorders like lupus and scleroderma
- conditions that lead to high platelet counts, such as essential thrombocythemia
- hormonal issues leading to low VWF protein production, such as hypothyroidism
- conditions that cause VWF to be removed from the bloodstream, including some kidney cancers
- certain medications, including some antibiotics and anti-fungal agents.
Types of von Willebrand disease
There are three main types of VWD, denoted as type 1 through type 3, which differ in prevalence, severity, and in the way they are inherited.
Type 1
In VWD type 1, VWF protein levels are lower than normal, but are still detectable. This is the most common type of VWD, affecting up to 85% of people who are treated for the condition, but it is also generally the mildest form of the disorder.
VWD type 1 is usually inherited in an autosomal dominant manner. However, this type of VWD is incompletely penetrant, meaning that the presence of the mutation doesn’t fully guarantee that a person will experience symptoms. It’s estimated that about 40% of people carrying a disease-causing mutation associated with VWD type 1 won’t have any disease symptoms.
Type 1C is a subtype of VWD type 1 where the VWF protein is made normally, but it is cleared out of the bloodstream too quickly. It manifests similarly to type 1, but it responds differently to a common VWD treatment called desmopressin.
Type 2
VWD type 2 occurs when mutations lead to the production of an abnormal form of the VWF protein that doesn’t work correctly. There are four subtypes of VWD type 2, based on the specific ways in which the protein is altered:
- type 2A, where the VWF protein cannot properly connect with other VWF proteins and form multimers and/or multimers are broken down too rapidly
- type 2B, where the VWF protein binds with abnormally increased affinity to another protein called GPlb on platelets, even in the absence of an injury
- type 2M, where the VWF protein doesn’t correctly bind to proteins on platelets
- type 2N, where the VWF protein doesn’t correctly interact with FVIII.
VWD type 2 is less common than type 1, but more common than type 3. It is also generally more severe than type 1, but milder than type 3.
VWD types 2A, 2B, and 2M are usually inherited in an autosomal dominant manner, while VWD type 2N is inherited in an autosomal recessive way.
Type 3
VWD type 3 is the rarest inherited form of the condition, affecting less than 10% of people with the disease. It is also generally the most severe form of VWD, often marked by frequent and severe bleeding. People with VWD type 3 are most likely to need routine prophylactic VWF replacement therapy to reduce the risk of serious bleeds.
VWD type 3 develops due to mutations that cause patients to have very low or no VWF. It is inherited in an autosomal recessive manner.
Diagnosis
VWD may be difficult to diagnose and go undetected in people who have mild symptoms. A VWD diagnosis generally involves assessing a person’s symptoms, medical and disease family history, followed by a combination of blood tests. These can include:
- tests to measure VWF levels
- tests to assess the activity of the VWF protein, its structure, and how it interacts with other clotting proteins like FVIII
- tests to assess how well platelets stick to each other to form clots
- tests to assess the levels and activity of other clotting proteins and evaluate the blood’s ability to clot and how long it takes for that to happen
- a complete blood count, which measures the numbers of platelets and blood cells.
Some of these tests may have to be repeated at different times due to fluctuations in VWF levels that can happen as a result of stress, exercise, pregnancy, the use of birth control medications, and other factors.
Ordering the correct tests and interpreting them appropriately is crucial for distinguishing VWD from other bleeding disorders that may cause similar symptoms. Based on the results of these tests, clinicians can generally identify VWD and pinpoint the specific type of disease a person has. Broadly, VWD is diagnosed when VWF protein activity is less than 30% of normal values.
Genetic testing to identify disease-causing mutations in the VWF gene is not generally required to confirm a VWD diagnosis, but genetic testing may be used in some cases to confirm the diagnosis and inform genetic counseling.
Symptoms and complications
For most people with VWD, symptoms are relatively mild. VWD symptoms can include:
- frequent, often spontaneous nosebleeds
- prolonged and excessive bleeding from cuts and scrapes
- bruising easily and often
- unusual bleeding following surgery or childbirth
- heavy menstrual bleeding
- blood in stool or urine.
Rarer, more serious complications of VWD can include:
- bleeding into the gastrointestinal tract
- bleeding into joints, leading to swelling, pain, and joint damage
- hematomas (blood pooling outside blood vessels)
- iron-deficiency anemia
- development of antibodies against some VWD treatments, which can make them less effective and increase the risk of serious allergic reactions.
Treatment and management
Several therapies can be used to manage VWD. Common VWD treatment options include:
- desmopressin, which increases VWF protein levels and is often used to manage milder bleeds in some people with VWD types 1 and 2
- VWF replacement therapies, which work by supplying a functional version of the VWF protein and are often used to manage more serious bleeds; they may also be given routinely as prophylaxis to prevent bleeds in patients with severe forms of VWD
- antifibrinolytics, which promote clotting by preventing the breakdown of blood clots and may be used to help manage bleeding in certain situations, including surgery or following childbirth
- birth control interventions, including birth control pills and intrauterine devices that may be used to help manage heavy periods.
In addition to these medications, lifestyle changes are often a part of living with VWD. In particular, patients are generally advised to take practical precautions to minimize the risk that they will be injured in a way that could lead to uncontrolled bleeding.
Bleeding Disorders News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.