Thrombotic thrombocytopenic purpura treatment
Last updated July 18, 2025, by Marisa Wexler, MS
 Fact-checked by Joana Carvalho, PhD
Fact-checked by Joana Carvalho, PhD
Thrombotic thrombocytopenic purpura (TTP) is a blood disorder marked by fever, low platelet counts, red blood cell destruction, and problems with the kidneys and nervous system.
TTP is considered a medical emergency. Without treatment, about 90% of people with TTP will die from it. But with appropriate care, the risk of mortality drops to about 10% to 15%. Outcomes are best when treatment is started as soon as possible.
All cases of TTP are marked by a reduced activity of an enzyme called ADAMTS13, which normally helps regulate blood clotting. Low ADAMTS13 activity leads to the excess formation of clots inside blood vessels, which drives disease symptoms. The two main types of TTP are:
- acquired TTP, also known as immune-mediated TTP, the most common form of the disease that occurs when the immune system produces antibodies that prevent the ADAMTS13 enzyme from working correctly
- congenital TTP, a rare form of the disease where reduced ADAMTS13 activity is caused by mutations that are present at birth.
Treatments for TTP broadly seek to normalize ADAMTS13 activity, preventing the excessive formation of blood clots and alleviating disease symptoms.
Main treatments
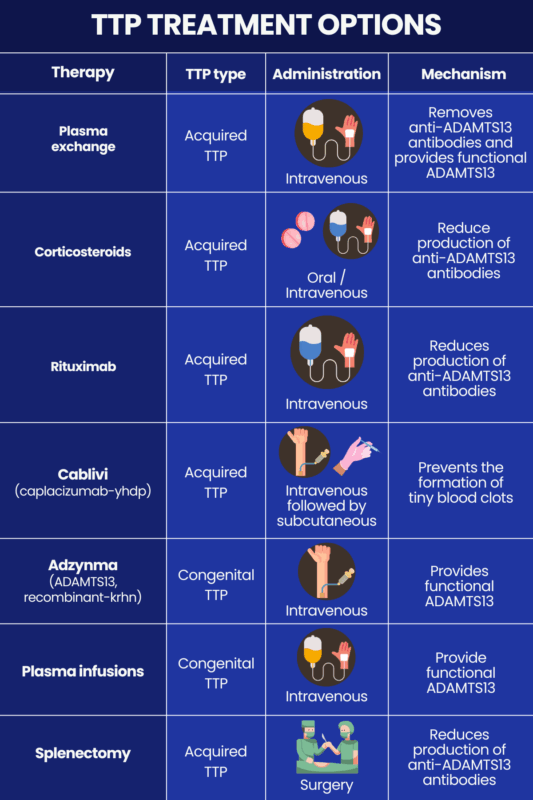
The main treatments used for TTP management are plasma exchange and corticosteroids. Current guidelines recommend these two treatments be given in combination to manage the first acute episode, as well as acute TTP relapses, that is, episodes where symptoms suddenly reappear or worsen after a period of remission, in patients with acquired TTP.
Plasma exchange
Plasma is the liquid portion of blood that doesn’t contain cells. It consists mostly of water, along with antibodies, and other proteins that circulate in the bloodstream. Plasma exchange — also referred to as PEX, PLEX, and TPE (short for therapeutic plasma exchange) — is a medical procedure wherein a person’s plasma is removed and replaced with healthy donor plasma. During the procedure, a needle or catheter draws the patient’s blood into a machine that separates out the plasma. The removed plasma is discarded and the blood cells are mixed with the donor plasma before being returned to the patient.
Because healthy plasma contains functional ADAMTS13, PEX can help restore the enzyme’s activity. In people with acquired TTP, plasma exchange also helps remove the harmful self-reactive antibodies that target ADAMTS13 and drive the disease.
Plasma exchange for TTP is usually given daily until platelet counts and other blood parameters normalize.
Corticosteroids
Corticosteroids are medications that have powerful immune-suppressing effects. They can be used to help reduce the production of the antibodies that drive acquired TTP.
There isn’t a single standard dosing regimen for corticosteroid use in TTP, though several may be used, including:
- oral prednisone at a dose of 1 mg/kg per day
- intravenous methylprednisolone at 1,000 mg per day or 125 mg two to four times daily for the first few days of treatment, in more severe cases.
Corticosteroids for acute TTP treatment are generally continued for as long as the patient is undergoing PEX, that is, until TTP symptoms subside and blood tests normalize. Suddenly stopping corticosteroid treatment can lead to a dangerous withdrawal syndrome. As such, patients who are ready to stop taking corticosteroids will slowly decrease their dose over several days or weeks before discontinuing the medication.
Other therapies
In addition to PEX and corticosteroids, several other treatments may be used to help manage TTP, including:
- rituximab and other immunosuppressive therapies
- Cablivi (caplacizumab-yhdp)
- Adzynma (ADAMTS13, recombinant-krhn)
- plasma infusions
- splenectomy.
Rituximab
Rituximab is an infusion therapy that works to lower the number of B-cells, the immune cells responsible for making antibodies. By depleting them, rituximab can reduce the production of the autoantibodies that drive acquired TTP. Despite not being specifically approved for TTP, rituximab has been increasingly used off-label for that purpose in recent years.
Current guidelines recommend that rituximab be used alongside PEX and corticosteroids to manage acute events (first episode and relapses) in people with acquired TTP. For people with acquired TTP who are in remission but still have low ADAMTS13 activity, the guidelines recommend rituximab be administered routinely as a prophylactic treatment to prevent relapses.
Other immunosuppressive therapies
In cases where PEX, corticosteroids, and rituximab are not sufficient for controlling acquired TTP, other immunosuppressive medications may be considered, although evidence supporting their effectiveness is limited. Examples include:
- cyclophosphamide, typically a single dose administered as an intravenous infusion
- cyclosporine A, which may be taken orally or administered into the bloodstream at various dosing schedules
- vincristine, typically a single dose administered as an infusion into the bloodstream.
Cablivi
Cablivi is an approved injectable therapy for acquired TTP. It is specifically approved to be used in combination with PEX and immunosuppressive treatments. It works to prevent the formation of the tiny clots that drive TTP by targeting a protein involved in blood clotting called von Willebrand factor.
Current guidelines recommend that Cablivi be used in people with acquired TTP who are experiencing an acute disease event.
The first dose of Cablivi is given by injection into the bloodstream, with subsequent doses being given by injections under the skin. The first dose is given when PEX is initiated, with treatment maintained for 30 days after the final round of PEX.
Adzynma
Adzynma is an approved enzyme replacement therapy for congenital TTP. The therapy is given by intravenous injection and works by providing a recombinant, or lab-made, version of the ADAMTS13 enzyme that is missing in people with congenital TTP. It may be used as a regular prophylactic treatment to prevent acute events, or on demand to manage an acute disease event in people with congenital TTP.
Current guidelines recommend that enzyme replacement therapy is preferred for patients with congenital TTP who are in remission over plasma infusions to prevent acute disease episodes.
Plasma infusions
Plasma infusions are a type of plasma therapy that involve administering healthy plasma into a patient’s bloodstream. Conceptually, this type of treatment is very similar to PEX, but lacks the initial step of removing a patient’s own plasma before adding in healthy plasma. Because people with congenital TTP do not have disease-driving antibodies that need to be removed, plasma infusions — which supply a functional version of the missing ADAMTS13 enzyme — are more commonly used than plasma exchange.
Routine plasma infusions were historically a mainstay congenital TTP treatment. Nowadays, enzyme replacement therapy is generally preferred when available because it is associated with a lower risk of potential complications, such as allergic reactions and infections. However, plasma infusions may still be used in some circumstances.
Splenectomy
The spleen is an organ that’s part of the immune system. In acquired TTP, the spleen is a major site of antibody production.
Splenectomy, or surgery to remove the spleen, has historically been used as a TTP treatment. Nowadays, however, it is rarely used because it is a major surgical procedure and other, less invasive treatments are usually effective. Still, splenectomy may be used in some cases where standard treatments aren’t effective.
Supportive care and monitoring
People with TTP who are experiencing an acute disease event are often managed in a facility with critical/intensive care capabilities to carefully monitor their condition during treatment. This includes:
- assessments of blood parameters and oxygen levels
- tests to evaluate heart health
- tests to assess neurological function.
In addition to treatments to manage TTP itself, patients also may benefit from supportive care to manage other conditions associated with TTP or to prevent certain complications. Supportive care in TTP may include:
- steps to prevent dangerous clots from forming in the legs, such as walking regularly or wearing compression stockings, once platelet counts have recovered
- treatments to keep blood pressure under control
- steps to prevent or minimize the risk of infections.
Long-term management and follow-up
A major goal of TTP treatment is to keep the disease in remission, meaning the patient is not experiencing any notable signs or symptoms of TTP. But even when the disease is in remission, there is a need for routine monitoring so any relapses can be quickly identified and treated.
In the long term, prophylactic treatment may be used to reduce the risk of relapses in people with TTP. This usually includes:
- rituximab for people with acquired TTP
- Adzynma, or plasma infusions if Adzynma is not available, for congenital TTP.
People living with TTP also will usually be counseled to try to avoid potential triggers of a TTP relapse. These may include:
- infections
- major injury or surgery
- use of recreational drugs like cocaine
- use of certain medications, including birth control pills, some cancer treatments, and certain medicines to prevent blood clotting
- pregnancy
- pancreatitis (inflammation of the pancreas).
Long-term TTP follow-up also generally involves routine tests to measure ADAMTS13 enzyme activity. If the enzyme’s activity is low (less than 10% of normal), then patients are at high risk of relapse and may be given additional treatments.
Living with a chronic illness like TTP can be stressful and take a toll on a person’s mental health. Thus, people with TTP may also benefit from emotional and psychological support, such as talk therapy or support groups. Some support groups for TTP include:
- TTP Support USA on Facebook
- Oklahoma TTP-HUS Support Group Meetings in Oklahoma
- The Ree Wynn Foundation in New Jersey
- Association ADAMTS13 in France
- Associazione Nazionale Porpora Trombotica Trombocitopenica (ANPTT) in Italy
- Japanese group for cTTP patients in Japan.
Bleeding Disorders News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.